
Acute Transverse Myelitis
Acute transverse myelitis (TM) is a rapid-onset immune-related spinal cord disorder often triggered by viral infections. It can lead to symptoms like weakness, sensory changes, and bladder problems. Treatment includes high-dose glucocorticoid therapy, plasma exchange in non-responsive cases, and supportive care like physical therapy and urinary retention management. Recurrence is possible, and some patients may develop multiple sclerosis, warranting chronic immunomodulatory therapy.
Introduction to Acute Transverse Myelitis (TM)
Acute transverse myelitis (TM) is an immune-mediated spinal cord disorder which could present with a rapid onset of weakness, sensory alterations, and bowel or bladder dysfunction. TM usually occurs as a postinfectious complication to viral infections, such as enteroviruses, mycoplasma, or treponema pallidum infections. It also exists on a continuum of neuro-inflammatory disorders which includes acute disseminated encephalomyelitis, neuromyelitis optica spectrum disorder, multiple sclerosis, and acute flaccid myelitis.
Subtypes of TM
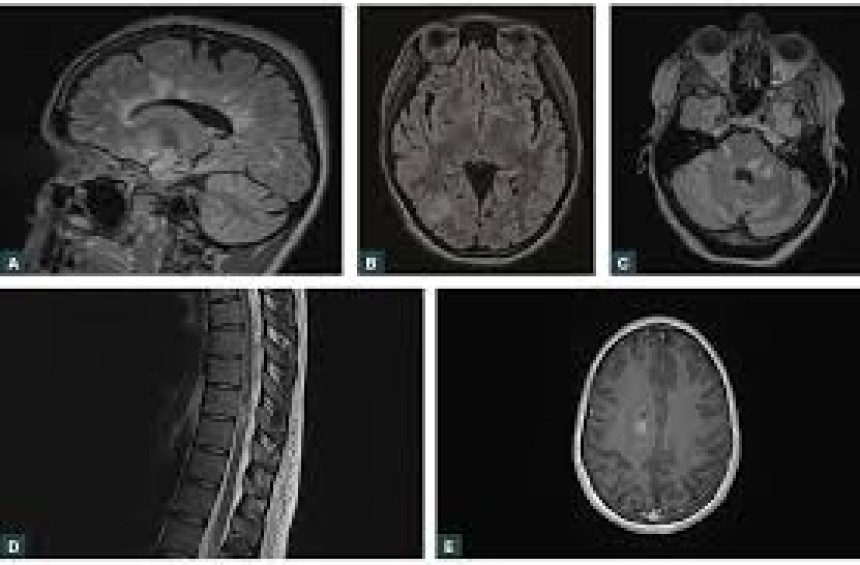
There are several subtypes of TM, including acute partial TM, acute flaccid myelitis (AFM), longitudinally extensive transverse myelitis (LETM), acute complete TM, and secondary TM. Secondary TM is associated with other autoimmune disorders, such as sarcoidosis, systemic lupus erythematosus, mixed connective tissue disorder, or Sjögren syndrome. Spinal MRI typically shows hyperintense signal changes in T2 images.
Treatment of Acute TM
Treatment of acute (idiopathic) TM is with high-dose intravenous glucocorticoid therapy (methylprednisolone [30 mg/kg up to 1000 mg daily], or dexamethasone [120 to 200 mg daily] for three to five days). Plasma exchange or cyclophosphamide may be options for those who fail to respond to high-dose glucocorticoid treatment. The treatment of secondary TM due to autoimmune etiology is primarily directed at the underlying condition.
Recurrence and Risk of Multiple Sclerosis
Recurrence has been reported in 25% of patients with idiopathic TM. Patients with recurrent TM are treated with chronic immunomodulatory therapy, including mycophenolate or intravenous rituximab, with acute attacks typically treated with high-dose intravenous glucocorticoids.
Dosage Adjustments and Precautions
For patients on cyclophosphamide, mycophenolate mofetil, or rituximab, treatment adjustments are necessary based on blood count levels and renal function. Premedication and assessment for progressive multifocal leucoencephalopathy are important for patients on rituximab.
Supportive Treatment
Patients with TM usually require supportive treatment including physical therapy, bladder catheterization for acute urinary retention, deep vein thrombosis prophylaxis, and rehabilitation therapy. This consists of passive and active therapy to maintain limb range of motion, reduce spasms and risk of contractures, and minimize the risk of decubitus ulceration.
References
1-Transverse Myelitis Consortium Working Group. Proposed diagnostic criteria and nosology of acute transverse myelitis. Neurology. 2002 Aug 27;59(4):499-505.
2-de Seze J, Lanctin C, Lebrun C, et al. Idiopathic acute transverse myelitis: application of the recent diagnostic criteria. Neurology. 2005 Dec 27;65(12):1950-3.
3-Jacob A, Weinshenker BG. An approach to the diagnosis of acute transverse myelitis. Semin Neurol. 2008 Feb;28(1):105-20.
4-Beh SC, Greenberg BM, Frohman T, et al. Transverse myelitis. Neurol Clin. 2013 Feb;31(1):79-138.
5-Cortese I, Chaudhry V, So YT, et al. Evidence-based guideline update: plasmapheresis in neurologic disorders: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2011 Jan 18;76(3):294-300.
6-Christensen PB, Wermuth L, Hinge HH, et al. Clinical course and long-term prognosis of acute transverse myelopathy. Acta Neurol Scand. 1990 May;81(5):431-5.
7-Krishnan C, Kaplin AI, Deshpande DM, et al. Transverse myelitis: pathogenesis, diagnosis and treatment. Front Biosci. 2004 May 1;9:1483-99.
8-Krishnan C, Kaplin AI, Pardo CA, et al. Demyelinating disorders: update on transverse myelitis. Curr Neurol Neurosci Rep. 2006 May;6(3):236-43.